Iowans Thrive Blog
Featuring stories, research, and news on Iowa's movement to respond to ACEs
|
|
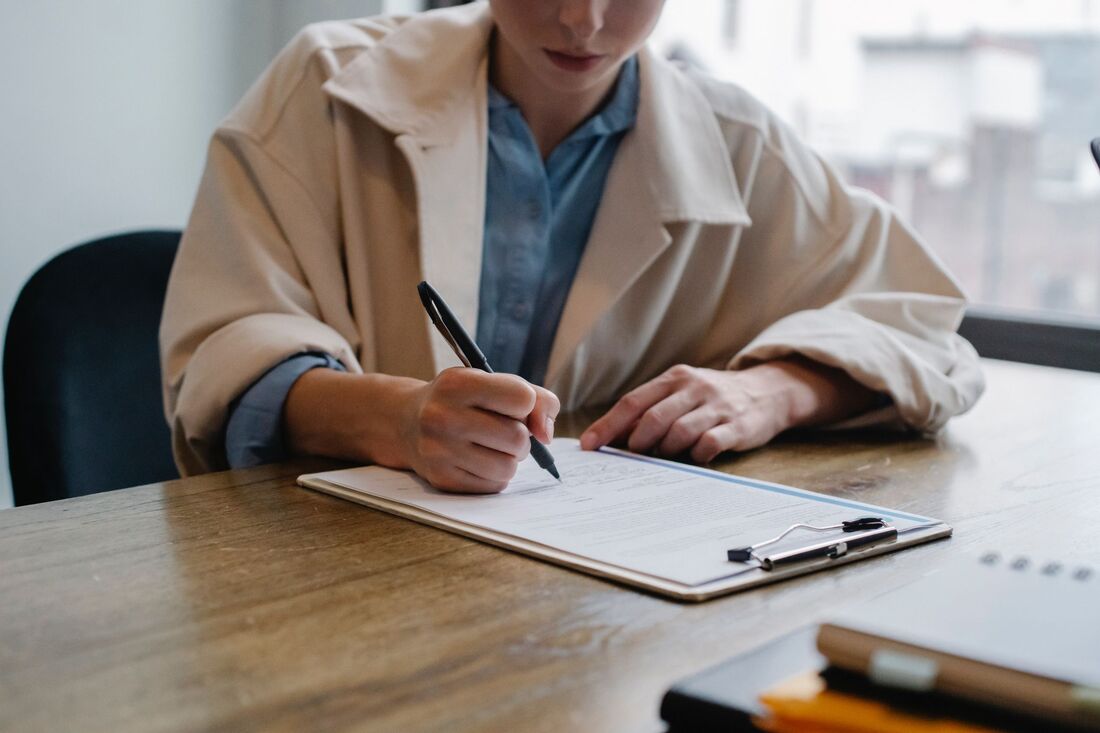 The Adverse Childhood Experiences (ACEs) Study was groundbreaking in that it showed a link between childhood trauma and adult health outcomes. The more types of childhood trauma adults reported experiencing, the greater their likelihood of having a wide range of health and mental health challenges, including anxiety, heart disease, substance use disorder, and diabetes. Iowa’s study, for example, shows that individuals with four or more ACEs are 5.3 times more likely to have COPD and 7.7 times more likely to have depression than those reporting zero ACEs. The ACE Study has spurred a movement focused on trauma-informed care, which considers what has happened to someone who may be experiencing challenges, rather than what is wrong with them. It also has led to using the ACE Study survey to measure individuals’ level of ACEs to better understand how past experiences may be influencing their current well-being. Knowing the connection between ACEs and adult outcomes is critical in working with individuals to heal from trauma and to prevent and mitigate ACEs in the future. Already, the ACE Study has inspired important policy and practice changes. But as we’ve learned more about the ACEs research, we also recognize that the ACEs survey should only be used within certain carefully established settings. Here are three reasons why sharing the survey with individuals may be problematic: 1. The ACEs survey was created to study population-level data. The 10-question ACEs survey was created to study the link between childhood trauma and adult health outcomes among a large population. Looking at the data among thousands of individuals allowed researchers to see the range of possible outcomes and to draw conclusions based on the median results. Using the survey to determine just one individual’s level of risk is problematic, because outcomes can vary widely from person to person. Someone may report high ACEs but not have any challenges. Others may report no ACEs and still face significant health issues. The chart below, shared in Dr. Robert Anda’s presentation on using the ACE survey, shows the range of possible outcomes as the ACE score (on the bottom of the image) increases. As the chart shows, there’s not a consistent distinction between ACE score and cumulative exposure to childhood stress for each individual, but we can draw conclusions looking at many scores. 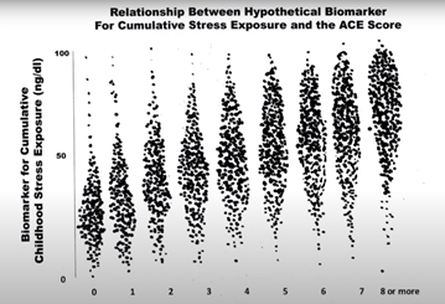 Outcomes can especially depend on the relationships a child had with adult caregivers, their connections in the community, the stability of their environment, and other resilience factors. For example, someone who experienced parental drug use and divorce as a child could also have had nurturing grandparents and teachers who helped buffer them from the full impact of the trauma. In fact, research shows that adults reporting 6-7 positive childhood experiences had 72% lower odds of suffering from depression or poor mental health, compared with those reporting 0-2 positive childhood experiences. Using four or more ACEs as a threshold for risk of negative outcomes may also be problematic. While experiencing four or more ACEs could indicate that someone has experienced a significant level of stress, research does not show that this is an absolute indicator. Most charts that present the ACE Study data use the 4+ marker simply to limit the size of the graph. The ACEs survey works best when used to study trends among several individuals to inform programming, policies, and systems. This article further explains why an ACEs score should not be used as an individual diagnostic measure. 2. The ACEs survey only considers 10 types of childhood trauma. Researchers decided to focus the ACE Study on just 10 types of trauma occurring within the home. Subsequent research has found that while a child may have a safe, stable, and nurturing home, they can still experience trauma within the community from situations like witnessing violence, bullying, and racist attacks. Individuals living in marginalized communities and in poverty especially experience trauma from the systems and environments they interact with. And over the past two years, many young people have experienced trauma as the pandemic has caused uncertainty, isolation, and stress. By only focusing on the 10 types of trauma on the ACEs questionnaire, we may miss significant trauma that someone experienced that is impacting them today. We may also miss the context in which household trauma has occurred, putting our focus on fixing families with problems, instead of working on the policies and systems that cause families to struggle. An individual’s level of ACEs matters less than knowing the science of early childhood development, which explains the link between how childhood adversity can affect future adult outcomes. The ACE Study and subsequent research further demonstrate the importance of focusing our responses on policies, systems, and practices that support families in providing nurturing environments for their kids. 3. Taking the survey without understanding or support can harm people. Asking individuals to complete the ACEs questionnaire may elicit strong emotions or expose deeper challenges, especially if people don’t have the full context of what the survey means and follow up support. Providers need to be prepared to have a thoughtful conversation with those taking the survey and to explain the results in a way that provides hope. Before drawing conclusions, providers should understand a person’s resilience and protective factors growing up, which could have helped buffer them from the impact of toxic stress, and be ready to refer people to local services and resources if someone needs additional support. In addition, we should be aware that families who are struggling are often asked to take a lot of assessments and to share painful and personal experiences many times. Repeatedly being asked questions about past trauma can be re-traumatizing. Being in a position of power as a doctor, therapist, or another kind of professional can make clients feel as though they have to take the survey when they don't want to. Instead, you might be able to glean information about past experiences by looking at what is already in a family’s file. Responding to ACEs must focus on root causes for trauma. The ACE Study shows us the importance of responding to all individuals with empathy and support and promoting conditions that support family well-being. Our policies and systems especially need to work toward helping people access essential needs and supportive connections within the community. If a caregiver is experiencing a high level of stress and is unable to access resources they need, their ability to be tuned in to their children and provide the best environment for their healthy development becomes more difficult. What to consider when administering the ACE survey The ACEs questionnaire can still be a valuable way to inform the work you do with individuals and families in some situations. If you choose to administer the ACE survey, we recommend you follow these guidelines:
Comments are closed.
|